DMEPOS Documentation Failures Are Costing Medicare $1.9 Billion Annually — Is Your Supplier Next?

Sofija Mamuchevski
Product & Growth Lead | AI Products | Demos, Outreach, Partnerships
Sofija Mamuchevski is Product & Growth Lead at DocuGenius, where she helps organizations modernize complex document workflows through automation, operational standardization, and compliance-focused processes. With more than 10 years of experience across software development, product management, and Agile delivery, she writes about document automation, operational efficiency, product strategy, and workflow transformation in regulated and document-heavy industries.
Reading time
7 min read
Published
June 17, 2026
CMS identified $1.9B in DMEPOS improper payments in FY2024. Learn why documentation failures drive denials and how suppliers can reduce audit risk.
$1.9 Billion. One Root Cause.
In Fiscal Year 2024, CMS identified $1.9 billion in DMEPOS improper payments — a 21.4% improper payment rate across the entire benefit category.
The dominant driver is not fraud. It is documentation — missing, incomplete, or insufficient records that make otherwise legitimate claims unpayable under Medicare rules.
For compliance directors, revenue cycle leaders, and billing managers, this is not an abstract policy problem. It is a direct threat to reimbursement, audit survival, and — when repayment demands follow — organizational solvency.
$1.9B / 21.4%
DMEPOS Improper Payments — FY2024 (Source: CMS Fraud Hot Spot)
Where the Losses Are Concentrated: FY2024 by Product Category
The risk is not uniform. CMS publishes improper payment data through its Comprehensive Error Rate Testing (CERT) program. Here is what FY2024 shows, category by category.
Continuous Glucose Monitors — $278 Million Lost to Documentation
CGMs carried the highest projected improper payment amount of any single DMEPOS item — approximately $278 million at a 25.2% improper payment rate. CMS confirmed the majority of errors stemmed from missing or insufficient documentation — not from equipment that was never delivered.
A beneficiary received the CGM. A physician ordered it. Medicare still denied the claim because the record failed to adequately document medical necessity.
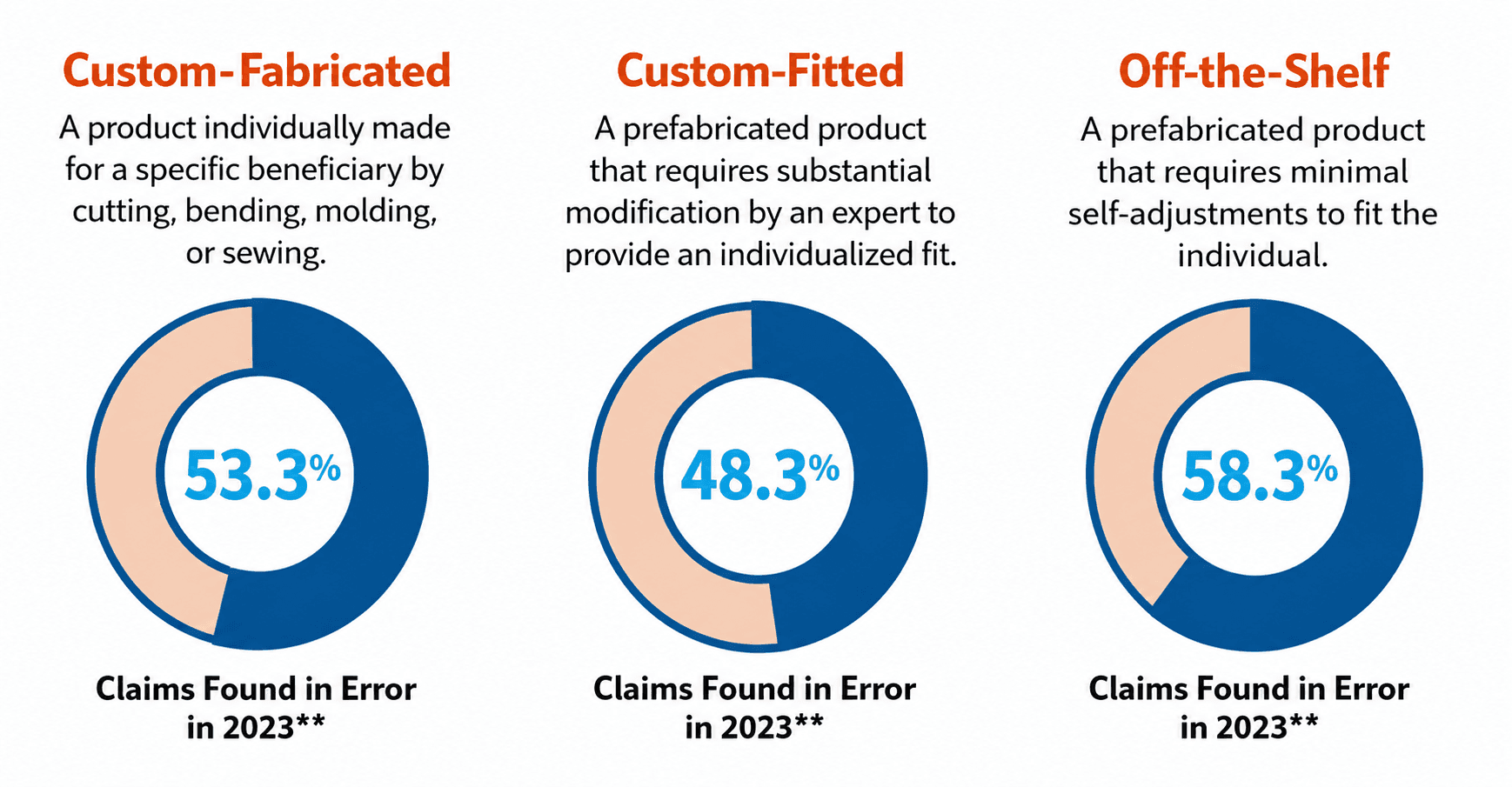
Orthotic Braces — More Than Half of All Claims Contain Errors
Orthotics produced some of the most alarming error rates in all of Medicare Part B. According to 2023 CERT data:
Custom-Fabricated orthoses: 53.3% of claims found in error
Custom-Fitted orthoses: 48.3% of claims found in error
Off-the-Shelf orthoses: 58.3% of claims found in error
The FY2024 improper payment rate for orthotics ranged between 35.2% and 54.4%. Any single missing element — the written order, the face-to-face encounter note, the clinical rationale — is enough for a denial.
Surgical Dressings — 57.6% Improper Payment Rate
Surgical dressings had the highest improper payment rate in the entire DMEPOS category at 57.6%, with projected improper payments of nearly $177 million.
More than half of every dollar billed for surgical dressings in FY2024 was flagged as an improper payment.
CMS flagged a specific risk pattern: suppliers billing large volumes of surgical dressings shortly after enrolling in Medicare draw heightened scrutiny from review contractors — regardless of whether the underlying billing is legitimate.
PAP Devices — Six Documentation Failures Driving $146M in Improper Payments
PAP devices (CPAP and bi-level) generated over $146 million in improper payments at a 12.5% rate. CMS identified six discrete failure modes behind these denials:
Missing clinical evaluation by the treating practitioner
No documentation that a sleep test was conducted
No proof of delivery of the device or supplies
Clinical evaluation does not assess the beneficiary for OSA
Additional documentation not produced when requested by auditors
Beneficiary already receiving a related device
Each failure maps to a specific gap in the documentation chain between the supplier and the referring practitioner’s office.
What CMS Actually Requires — And How the Rules Keep Expanding
The 6-Element Written Order Standard (Effective January 1, 2020)
Under Final Rule CMS-1713, every DMEPOS written order must contain all six elements. One missing field means the order is incomplete and the claim is at risk:
Beneficiary name or Medicare Beneficiary Identifier (MBI)
Description of the item
Quantity, if applicable
Treating practitioner name or NPI
Date of the order
Treating practitioner signature
For items on the Required Face-to-Face List, the complete order must exist prior to delivery — not merely prior to claim submission. That distinction alone disqualifies a large share of otherwise valid claims.
83 Items Now Require Face-to-Face Encounter + Written Order Prior to Delivery
CMS has expanded this list through four Federal Register notices since 2022:
Jan 2022 (87 FR 2051): 46 PMD codes + 7 additional items
Jan 2023 (88 FR 2546): 10 additional orthoses
May 2024 (89 FR 41324): 13 additional codes (hospital beds, osteogenesis stimulators, lumbar sacral and knee orthoses)
Jan 2026 (91 FR 1250): 8 oxygen and oxygen delivery system codes — effective April 13, 2026
As of April 13, 2026, there are 83 items on the Required Face-to-Face Encounter and Written Order Prior to Delivery List. This list did not exist in its current form four years ago.
Suppliers who have not updated their intake workflows to track this list by item code are billing into a compliance gap — often without knowing it.
Prior Authorization: An Expanding Parallel Requirement
Separate from the face-to-face requirements, CMS’s Required Prior Authorization List added nine HCPCS codes in 2024 and seven more in April 2026. Effective January 1, 2025, CMS reduced the standard prior authorization review window to seven calendar days. Suppliers with documented compliance track records may now qualify for a prior authorization exemption under CMS-1828-F — but demonstrating that record requires the same documentation infrastructure that most suppliers currently lack.
This Is a Workflow Problem, Not a Knowledge Problem
Most billing managers understand, in general terms, what Medicare requires. The error rates above are not caused by ignorance of coverage policy.
They are caused by operational friction at the boundaries between systems and organizations — the points where documentation is handed off, assumed to exist, or never collected at all.
Consider a single complex orthotic claim. The supplier must confirm the item is on the Required Face-to-Face List. Confirm a qualifying encounter occurred within the preceding six months. Obtain a complete six-element written order — before delivery, not before billing. Retain the order and supporting clinical documentation. Produce it within 45 days if a MAC Additional Documentation Request arrives.
In organizations using fax-based order intake and manual spreadsheet tracking, this chain breaks routinely. A practitioner’s office sends an order with no NPI. A face-to-face note exists in the EHR but was never transmitted to the supplier. A prior authorization number was obtained but never linked to the claim.
None of these failures are caught by billing system edits — because they are documentation completeness problems, not coding problems.
Audit Exposure Is Real — and Escalating
DMEPOS is an active priority across CMS’s entire review contractor ecosystem: MACs under Targeted Probe and Educate (TPE), Supplemental Medical Review Contractors (SMRCs), and Recovery Audit Contractors (RACs).
TPE reviews are particularly consequential. A supplier selected for a probe phase faces review of 20–40 claims. A high error rate triggers a second round, then a third — each with mandatory education. Suppliers who fail to improve after three rounds can be referred to CMS for further action, up to and including suspension from the Medicare program.
For a supplier whose workflows haven’t been updated to reflect the 2022, 2023, 2024, and 2026 expansions to the Required Face-to-Face List, the first sign of that gap may be a TPE probe — at which point the exposure is already realized.
Why Existing Tools Cannot Close This Gap
Manual Review Doesn’t Scale
A compliance coordinator checking paper orders against an 83-item Federal Register list is performing a task that is both error-prone and economically unsustainable at volume. Multi-variable checks — NPI present, encounter within six months, order received before delivery, prior authorization linked to claim — must happen on every claim, every time. Manual processes cannot deliver that consistency.
Billing Systems Operate Downstream of the Problem
Billing systems validate codes, modifiers, and eligibility. They do not evaluate whether a face-to-face encounter note documents beneficiary-specific subjective and objective clinical findings. They do not confirm whether a written order arrived before delivery or only before claim submission.
The $1.9 billion improper payment problem originates upstream of the billing system — in the order intake and documentation collection workflow. That is where the fix must happen.
How DocuGenius Addresses the Structural Gap
DocuGenius operates at the documentation layer — the point where most DMEPOS compliance failures originate — rather than replacing billing or clinical systems.
For DMEPOS suppliers, this means systematically validating incoming orders against the six-element CMS standard, cross-referencing ordered items against the current Required Face-to-Face List, and flagging documentation gaps before a claim is submitted — not after an audit letter arrives.
It also means being able to produce a complete, organized documentation package in response to an Additional Documentation Request within the required window — without a manual search across fax archives, filing systems, and practitioner offices.
In an environment where surgical dressings are denied at a 57.6% rate and orthotic claims fail above 50%, the difference between a sustainable DMEPOS business and an unsustainable one is operational — not clinical.
The suppliers who will perform best under CMS’s expanding documentation requirements are those who have solved this as a systematic capability rather than a periodic compliance project.
Primary Sources
CMS DMEPOS Order and Face-to-Face Encounter Requirements (modified March 4, 2026) — cms.gov
Federal Register Notices: 87 FR 2051, 88 FR 2546, 89 FR 41324, 91 FR 1250
Sofija Mamuchevski
Product & Growth Lead | AI Products | Demos, Outreach, Partnerships
Sofija Mamuchevski is Product & Growth Lead at DocuGenius, where she helps organizations modernize complex document workflows through automation, operational standardization, and compliance-focused processes. With more than 10 years of experience across software development, product management, and Agile delivery, she writes about document automation, operational efficiency, product strategy, and workflow transformation in regulated and document-heavy industries.